A simple and easy way to remember your anti-arrhythmic agents. Mnemonics: Some Block Potassium Channels.
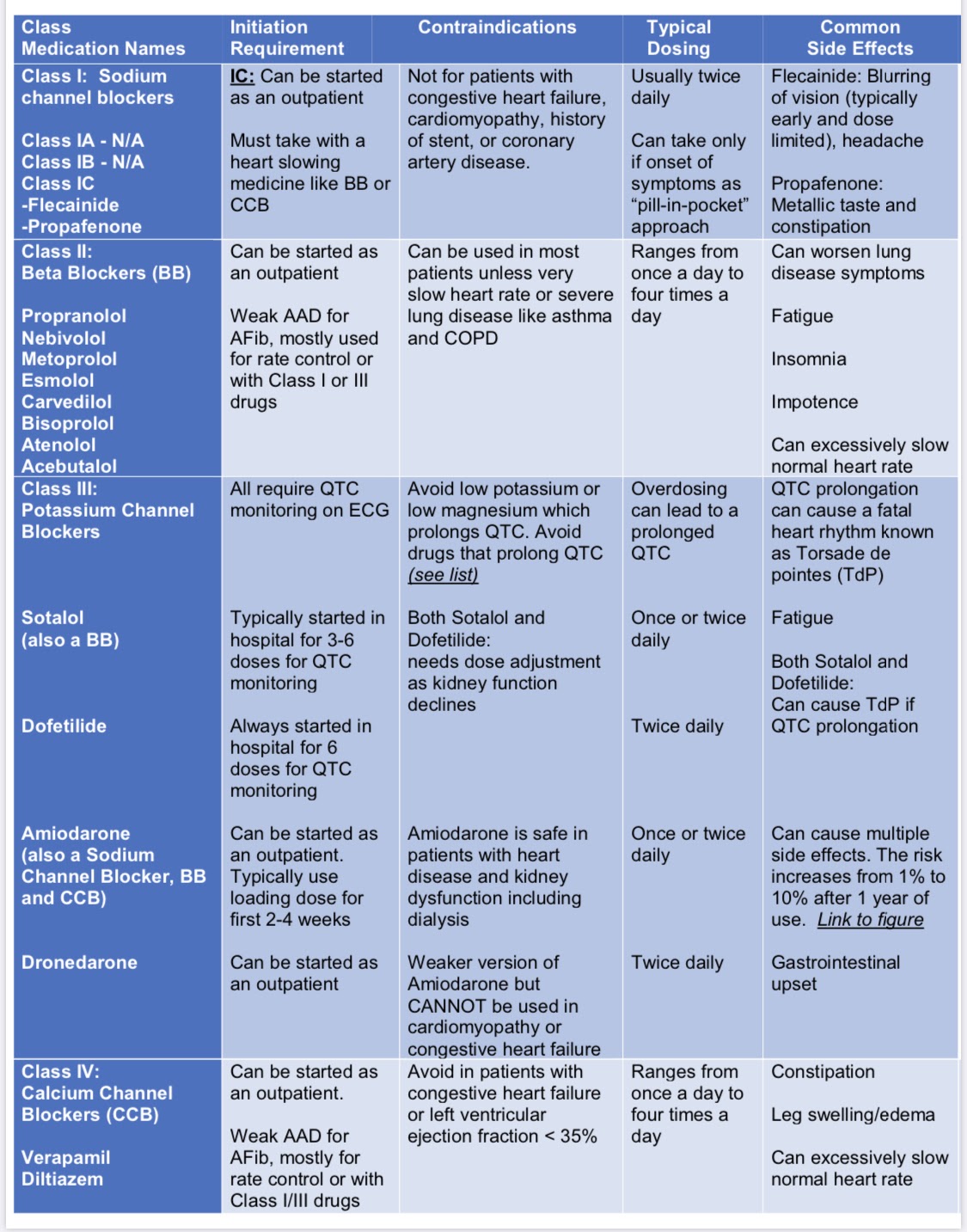
Vaughn-Williams Classification | Class I: Sodium Channel Blockers. Class II: Beta-Blockers. Class III: Potassium Channel Blockers. Class IV: Calcium Channel Blockers.
Class I
Class Ia: Causes moderate degree blockage of fast sodium channels. Drugs include quinidine, procainamide, and disopyramide. Causes prolonged QTc interval; use is limited due to pro-arrhythmic potential.
Class Ib: Causes mild degree blockage of sodium channels. Drugs include lidocaine and mexiletine. Shorten the QTc interval, are used for VA only, especially post-myocardial infarction VA, and are not useful for atrial arrhythmias. In long QT syndrome, mexiletine shortens the QTc interval and has been used to reduce recurrent and ICD arrhythmias.
Class Ic: Causes marked degree of sodium blockage and no effect on QT interval. Drugs include flecainide or propafenone. These drugs are reasonable for ongoing management in patients without structural heart disease or ischemic heart disease who have symptomatic supraventricular tachycardia (SVT) and are not candidates for or prefer not to undergo catheter ablation.
Class II
Beta-blockers (BB) are indicated for rate control in patients with paroxysmal, persistent, or permanent AF and atrial flutter. Oral beta-blockers are useful for ongoing management in symptomatic supraventricular tachycardia (SVT) patients. Beta-blockers are often first-line antiarrhythmic therapy because of their excellent safety profile and effectiveness in treating ventricular arrhythmias. Therapy with beta-blockers reduces adverse cardiac events for long QT syndrome and catecholaminergic polymorphic ventricular tachycardia.
Class III
Potassium channel blockers decrease potassium efflux out of the cell and prolong the QTc interval.
Class IV
Non-dihydropyridine calcium channel blockers (diltiazem, verapamil) decrease conduction velocity and slow conduction through the AV node. Ventricular rate control in acute and chronic AF and atrial flutter. Diltiazem and verapamil are options in the acute treatment of hemodynamically stable patients with SVT, focal, and multifocal atrial tachycardias
Refer to pocket guide anti-arrhythmic agents mechanism of action | anti -arrhythmic agents
Names, dates, and personal identifying details have been changed throughout this website to comply with the Health Insurance Portability and Accountability Act (HIPAA). ** | This website runs on coffee. Thank you for supporting this journey!

{kind=link}
Leave a comment