
Rapid response call: 05:20 am, A rapid response was called towards the end of the shift for a 56-year-old patient in the tele department for an acute desaturation event. He had a significant PMHX of colon cancer, DM 2 and COPD. The primary RN noted that the patient was on room air prior to NGT placement but received a call 5 minutes after the procedure from tele monitor tech that his saturation was sustaining in the 80’s. Pt was quickly positioned to a fowler and placed on 4, 5, 15 L 02 and eventually on HFNC. Despite supplemental 02, his oxygenation had very minimal response. His saturation sustained at 81% despite oxygen support. Pt was slightly tachypneic at 33, he felt fatigued but overall denied pain. His blood pressure remained stable. A quick NP-POCUS revealed a collapsible IVC on inspiration with no evidence of right heart strain, septal deviation or D sign. The CXR did not show any acute process. Pt continued to be coherent. He was cyanotic but continued to converse in complete unbroken sentences.
Upon further investigation it was noted by the primary RN that patient received a local anesthetic spray prior to his NGT placement. ABG revealed pH 7.41/Pa02 250 mmHg, methemoglobin level of 16%. His saturation gap is 6%.
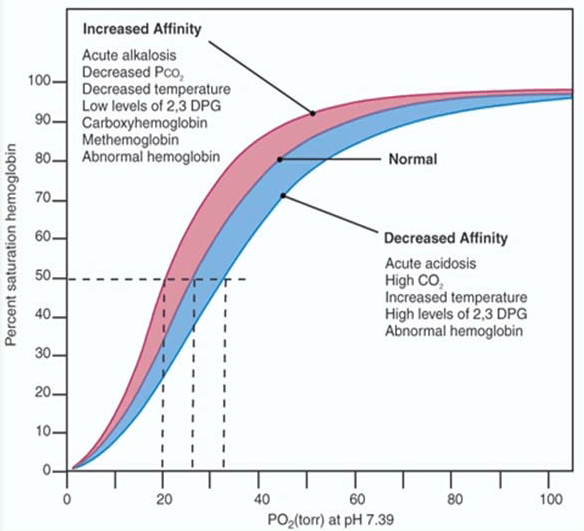
The patient was diagnosed with methemoglobinemia. This condition causes A shift to the left on the oxyhemoglobin dissociation curve. This indicates increased hemoglobin affinity for oxygen and an increased reluctance to release oxygen into the cells explaining his clinical presentation that’s puzzled the team after the arterial blood gas analysis. He was treated with Methylene blue of 1 mg/kg intravenously. His symptoms improved within 45 minutes of treatment.
Quick review on the oxyhemoglobin dissociation curve:
Hemoglobin (Hb) molecule is the combination of protein globin and nonprotein portion called haem and responsible for essentially transporting of the oxygen in the blood. Hemoglobin is composed of four subunits: two alpha subunits and two beta subunits, each of which contains a heme group and globin chain. The heme group contains an iron atom as ferrous form(Fe 2+) at its core that binds one oxygen molecule, allowing one hemoglobin tetramer to bind four oxygen molecules.[2] Hemoglobin exists in two states: the T (deoxygenated-tense) state and the R (oxygenated-relaxed) state. The two states differ in their affinity to bind oxygen. In an unbound state, hemoglobin exists in the T state, and binding of oxygen occurs with low affinity. The T-state hemoglobin thus requires a higher partial pressure of oxygen (pO2) to facilitate the binding of an oxygen molecule. The binding of single oxygen induces a conformational change that destabilizes the T state and facilitates the transition of the other subunits to the high-affinity R state. The binding of the first oxygen allows the second, third, and fourth oxygen molecules to subsequently bind with increasing ease. This relationship is an example of positive cooperativity.
A rightward shift of the curve indicates that hemoglobin has a decreased affinity for oxygen, thus, oxygen actively unloads. A shift to the left indicates increased hemoglobin affinity for oxygen and an increased reluctance to release oxygen.
- PH: decrease in pH (acidity) shifts the dissociation curve to the right while an increase in pH (alkalinity) shifts the dissociation curve to the left.
- CO2: an increase in hydrogen ions stabilize the hemoglobin in the T-state and induces oxygen unloading which leads to shifting of the dissociation curve to the right.
- 2,3-Diphosphoglycerate (DPG): intermediate product of glycolysis that is produced within the red blood cell. High concentrations of 2,3-DPG will shift the dissociation curve to the right whereas low concentrations will shift the curve to the left. The relationship of hydrogen ions is inversely proportionate with levels of 2,3 DPG.
- Temperature: Oxygen unloading is favored at higher temperatures which will cause a rightward shift. On the other hand, lower temperatures will cause a leftward shift in the dissociation curve. Exercise shifting the curve to the right and allowing oxygen to be more easily unloaded.
- CO: Hemoglobin binds carbon monoxide (CO) 200 to 300 times more than with oxygen, resulting in the formation of carboxyhemoglobin and preventing the binding of oxygen to hemoglobin due to the competition of the same binding sites. The binding of one CO molecule to hemoglobin increases the affinity of the other binding spots for oxygen, leading to a left shift in the dissociation curve. This shift prevents oxygen unloading in peripheral tissue and therefore the oxygen concentration of the tissue is much lower than normal. Thus in the presence of carbon monoxide, a person can experience severe tissue hypoxia while maintaining a normal PaO2. Patients with CO poisoning experience symptoms such as headache, malaise, altered mental status, shortness of breath, seizures, or cherry red lips. A pulse oximeter would usually be normal because the machine is unable to detect carboxyhemoglobin from oxyhemoglobin.
- Fetal hemoglobin (HbF) is structurally different than adult hemoglobin because it is composed of two alpha and two gamma chains. The gamma chains of HbF have a reduced affinity for 2,3-DPG, thus allowing HbF to have a higher affinity for oxygen at lower levels of partial pressure and resulting in a leftward shift of the dissociation curve. This state is advantageous in the womb, as the fetus can pull oxygen from maternal circulation with greater ease. At the level of the placenta, 2,3-DPG interacts more readily with adult hemoglobin, inducing oxygen unloading. Whereas, fetal hemoglobin is unaffected by the 2,3-DPG and can bind oxygen easily.
Saturation gap is the difference between SpO2 calculated by ABG and the Spo2 measured by pulse oximetry. Difference of more than 5% is a positive saturation gap.
Names, dates, and personal identifying details have been changed throughout this website to comply with the Health Insurance Portability and Accountability Act (HIPAA). **

Thank you Elijah for this post. This is a great case study to share with students and staff.
LikeLiked by 1 person
I appreciate it David!
LikeLike