RIVERSIDE, Calif., September 21, 2023 /Business Wire/ — Riverside University Health System is proud to announce the implementation of FloPatch by Flosonics Medical. As a pioneer in adopting new, ground-breaking medical technology, Riverside is making a significant leap forward in healthcare innovation, particularly in the life-saving area of sepsis management. read more. Hi everyone. Here is... Continue Reading →
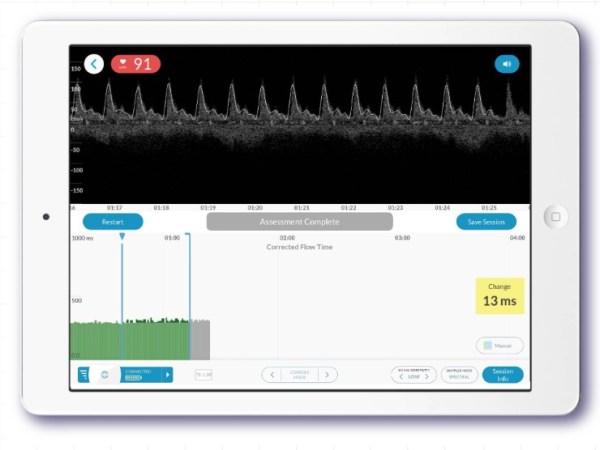
Quick Flopatch overview